AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2578-8949/012
*Corresponding Author: Diego Luis, Department of Dermatology, Germany.
Citation: Diego Luis, Ethan Nicholas,Kaden Riley and Samuel James, Lipedematous Scalp and Lipedematous Alopecia with Unknown Etiology and Pathogenesis. J .Dermatology and Dermatitis. Doi: 10.31579/2578-8949/012
Copyright: © 2017 Diego Luis. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 September 2017 | Accepted: 25 September 2017 | Published: 30 September 2017
Keywords: lipedematous scalp; scalp; hair; hyperlipidemia; alopecia
Lipedematous scalp and lipedematous alopecia is characterized by the localized accumulation of fatty tissue in the subcutaneous layer of the scalp. However, there is no effective treatment for this slowly progressing condition. Here we report the first case in the medical literature of spontaneous resolution of lipedematous scalp in a patient whom we diagnosed and reported in 2004 to have Lipedematous scalp.
Lipedematous scalp (LS) is a condition in which there is localized accumulation of fatty tissue in the subcutaneous layer of the scalp without hair abnormalities. While lipedematous alopecia (LA) is a condition in which there is localized accumulation of fatty tissue in the subcutaneous layer of the scalp associated with alopecia. It is still unclear whether LS and LA are separate entities or variable expressions of the same disease. Clinically it is detected by palpation of the scalp exhibiting a localized soft and non-tender swelling. Currently, there is no effective treatment for LS but surgical treatment and oral mycophenolate mofetil were documented to to be effective in LA as single case reports [1,2]. Here we report the first case in the medical literature of spontaneous resolution of lipedematous scalp in a patient whom we diagnosed and reported in 2004 to have Lipedematous scalp [3].
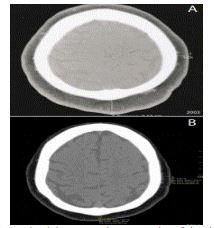
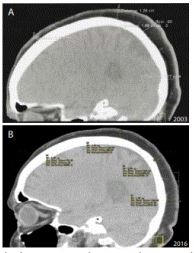
A 69-year-old southern Arabic female presented to our dermatology clinic at King Fahd Hospital of the University as a follow up case of lipedematous scalp diagnosed in our clinic in 2003. She is a known case of supraventricular tachycardia and hypercholestermia well controlled with medication. Besides, the patient scalp condition was last evaluated four years prior to her current visit in our clinic with no significant change. Interestingly, on examination of the scalp, there was absence of the spongy feeling on palpation and there was no loss of hair. Routine blood and biochemical tests, lipid profile and thyroid profile were normal. Axial computed tomography of the skull showed scalp thickness in the high occipitoparietal region of 8 MM as compared to 21.1 mm in 2003. (Figure1 A,B) while midsagittal reconstructed computed tomography showed a scalp thickness at the high occipitoparietal region of 9 mm as compared to 16.9 mm in 2003. (Figure2 A,B) Subcutaneous fat thickness was almost 6 mm at the occipitoparietal region which is normal compared to 19.2 mm reported in 2003 for the same region. So we confirmed our impression of spontaneous complete resolution of lipedematous scalp after thirteen years duration.
The word lipedema per se means accumulation of excess fat and fluid in the subcutaneous tissues. Lipedematous Scalp and Lipedematous alopecia are two scalp conditions that have similar clinical morphology, imaging features and course. Clinically both present as soft, spongy or doughy scalp on palpation initially localized at the vertex and occipital areas and slowly expand to involve the entire scalp. There may be associated symptoms of pain, paresthesias, headache, burning sensations, tenderness, or pruritus [3]. There are 50 published cases of LS and LA in the literature with female predominance and mean age of onset of 42 years [3-5]. Magnetic resonance imaging is the best diagnostic method with deep incisional biopsy [6]. Additionally, puncture with sterile needles, computed tomography of the head or ultrasound can be used to measure the scalp objectively [7]. Basically, the normal scalp thickness in an adult person is about 5-8mm [8,9]. While pathologic scalp thickness is reported to be 9 to 19 mm [7,10]. As for our patient the scalp thickness decreased to approximately 6 mm.
The mechanism underlying the pathogenesis of LA or LS remains unknown. Leptin has been suggested as a candidate hormone in the pathogenesis of LA and LS [1]. It is known to be involved in fat distribution and lipoapoptosis. On the contrary, Jone et al. [11], suggested adipose metaplasia and developmental displacement of adipose tissue or possible origin of adipocytes from the wall of dermal vessels in the course of degenerative changes in dermal connective tissue as recently reported an association of LA with discoid lupus erythematosus has been proposed [11,12]. Regarding the associated alopecia, Martin et al postulated the presence of lymphangiectasia may be responsible for hair loss because it is found only in those patients with lipedematous scalp and alopecia [13]. Others relate alopecia to compression of the superficial blood capillaries by the increased volume of the subcutaneous fat layer within the thickened scalp. In the present case the scalp thickness was 8-9 mm in the high occipitoparietal region compared to 21.1-16.9 mm in 2003 with subcutaneous fat layer reduced significantly to 6 mm after it was 19.2 mm [3]. We could not explain the resolution of the condition except that it is spontaneous. Currently, there is no effective treatment for LS or LA. Systemic and intralesional steroids have been utilized with no clear effect [14]. Yip et al. [1], reported a successful treatment of LAS by surgical intervention with debulking and scalp reduction. Caberera et al. [2], reported successful treatment of LS using mycophenolate mofetil. Our case is the first reported case of LS resolving spontaneously after 13 years which adds a significant clinical prognostic value to LS and LA. Further follow up of the previously reported cases in the literature is highly recommended to support our observation of spontaneous resolution of LS.
Lipedematous scalp and lipedematous alopecia is two rare dermatological disorders with unknown etiology and pathogenesis with no consistent systemic comorbidity. Up to date, only 50 cases have been reported in the world and our case is the first case among them that showed complete resolution. Future studies are needed to reveal the pathophysiology behind this rare disorder.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.



























































